
Even before the COVID-19 pandemic, loneliness was gaining increasing attention as something highly relevant for our health and well-being. In times of social distancing and lockdowns all over the world, the topic is even more present. Researchers has tangled with the question of how best to help people suffering from frequent feelings of loneliness. A highly cited meta-analysis by Masi and colleagues (2011) found that interventions aimed at addressing unhelpful thoughts and cognitive tendencies regarding social situations seemed to work the best and named cognitive behavioural therapy (CBT) a potential candidate for helping the lonely. Below we take a look at a study by Lindsay et al. (2019) investigating the use of mindfulness, often incorporated in third-wave CBT therapies, as a tool to help people feel less lonely.
In line with the findings from the meta-analysis by Masi et al (2011), some researchers have looked into the possibility of using techniques found in CBT treatments for psychiatric disorders and mental health problems as a way of reducing loneliness. The idea of using methods and techniques found in psychological treatments ties into research findings on how loneliness is related to changes in many cognitive and perceptual processes (Spithoven, Bijttebier & Goossens, 2017). The lonely person may not only experience significant emotional distress, but also perceive the social world in a different way than a person that does not feel lonely. As an example from their systematic review, Spithoven and colleagues (2017) described that people with high ratings of loneliness may interpret social situations as more threatening than their non-lonely peers. These unfortunate tendencies may in turn lead to an increased isolation and fewer attempts at reaching out for that valuable social connection that is sorely needed. From this comes the idea that mitigating the impact that loneliness can have on one’s cognitive processes and perception could be a way of helping people break out of their loneliness and increase their sense of connection with others.
Could mindfulness help with this? Staying in the present moment and adapting a non-judgmental stance towards the thoughts and feelings we encounter throughout the day is thought to help reduce the sway that painful emotions and experiences can have our mood and behaviours. The concepts and techniques included in mindfulness-based therapies have also gained support in well-designed studies as a way of reducing stress and mental health problems (Khoury et al., 2013).
Tying together loneliness and the use of mindfulness, Lindsay and colleagues (2019) sought to investigate whether techniques found in the mindfulness arsenal could help reduce loneliness. The authors hypothesised that using mindfulness as a tool for regulating one’s emotional responses could be helpful in the case of loneliness due to its link with the maladaptive perceptual and cognitive tendencies mentioned above. Reducing the perception of threat in these situations was also thought to improve one’s social functioning, allowing for a more fulfilling participation in the social world. In addition to testing whether mindfulness could help reduce loneliness, the authors also looked to investigate the benefits of staying in the present moment (the monitoring component) relative to the benefit of an accepting attitude towards the potentially unpleasant and unwelcome experiences encountered (the acceptance component). Would removing the latter undo the expected effects? The authors speculated that acceptance was a necessary ingredient and that removing this component would negate the benefits of the mindfulness approach in reducing loneliness.

Research has suggested that loneliness is related to many cognitive processes that affect how we perceive and experience social situations.
Methods
The authors looked to test their hypotheses using a three-group design. Participants were randomised to receive training in mindfulness (known as the monitoring condition), to receive training in mindfulness along with training in promoting an accepting stance towards thoughts and sensations (known as monitoring + acceptance) or analysing one’s thoughts and feelings (known as the coping condition). Participants were recruited as part of a larger study interested in looking at the effects of guided mindfulness on stress. Due to this, all participants included reported moderate-to-high levels of stress, though loneliness levels were not used as an inclusion criterion. In total, 153 participants took part in the study.
The intervention was accessed through a smartphone app and spread out over 14 lessons provided daily with audio-recorded guidance. One part of the programme, monitoring, focused on paying attention to the present moment, noticing thoughts, feelings and bodily sensations and discriminating between these. The additional acceptance content focused on maintaining a sense of relaxation, welcoming sensations and experiences felt in the body, and labelling these with a neutral tone. The control group in the coping condition received instructions for common techniques used to analyse, reappraise and cope with the thoughts and feelings encountered throughout the day. They did not receive any of the content related to mindfulness or acceptance. All of the groups took part in their respective programme for 14 days.
Loneliness was measured in two ways, though the results of only one of them are presented in the main paper while the other one is reserved for the online appendix. The researchers measure daily loneliness using ecological momentary assessment (EMA) before and after the participant completed their programme. In the evenings during the 14-day programme, participants would be prompted to indicate how lonely they had felt during that day on a seven-point Likert scale ranging from Not at all to Extremely. In addition to the daily ratings of loneliness, participants also completed the commonly used UCLA Loneliness Scale as a measure of what the authors labelled as retrospective loneliness. Participants completed these ratings in the lab prior to and after the intervention.
In addition to loneliness, the perception of being socially isolated, the authors also wanted to look at whether the mindfulness programmes led to an increase in objective social contacts during these two weeks. This was done using EMA prompts asking the participants about the numbers of social interactions they had have since last time they were asked the question and with whom they had been interacting.
Results
For ratings of daily loneliness, the results were in line with the hypothesis that the authors set up prior to the study. The monitoring + acceptance condition did see a reduction in loneliness (mean change in daily loneliness = −0.49, p = 0.0001, d = 0.44), while both the monitoring (mean change = 0.02, P = 0.837, d = −0.02) and the control condition mean change = 0.00, P = 0.981, d = −0.01) experienced no significant change after the 14 days.
Interestingly, the same pattern was not found for the measure of retrospective loneliness. Here, the results indicated that none of the groups changed significantly more than the others, (Time by group interaction: χ2(2)=1.63, p = .442). The change within the groups did point to significant reductions across all groups, with effect sizes between d = .40 and d = .67. However, for this measure, the control condition actually saw the largest reduction from the assessment before the intervention to the one after.
The results for the objective measure of social isolation was in line with the ones found for the primary measure of daily loneliness. The group training in both mindfulness and acceptance saw an increase of social interactions (mean change in number of interactions = 0.40, p = 0.001, d = 0.31). Neither the monitoring condition (mean change in number of interactions = −0.06, p = 0.622, d = −0.04), nor the coping condition (mean change in number of interactions = 0.02, p = 0.914, d = 0.02) experienced a change after receiving their respective intervention.

Participants trained in both monitoring and acceptance saw a decrease in daily loneliness.
Conclusions
In relation to the questions posed by the authors, two conclusions can be drawn from the results: mindfulness interventions may help reduce daily feelings of loneliness, but this may only be the case when the practice involves both awareness of the present moment and training in acceptance. The main findings were in line with the hypothesis specified by the authors. Whether or not the lessened feelings of loneliness are caused by the hypothesised increase in social functioning remains to be investigated. The reduction in daily loneliness was also accompanied by an increase in social interactions, though it is unclear whether this increase lead to a decrease in loneliness or the other way around.
The discrepancy between the findings for the measures of daily loneliness and retrospective loneliness is interesting as many studies in the past investigating methods of reducing loneliness have either used the UCLA Loneliness Scale or measures relying on the same type of retrospective reporting. Which option is the best, remains to be investigated.
Strengths and limitations
A definite strength of the study was the authors use of three active conditions to test their hypotheses. Giving all the participants access to some kind of active psychological exercises and techniques generally serves as a tough test. This is also great for ruling out potential placebo effects that might occur simply due to the fact that the participants actively participate in something they consider to be related to their mental health.
As noted by the authors in the article, a limitation was the fact that the participants in the study were not recruited based on feelings of loneliness, but rather based on stress levels. Due to this, it is hard to judge whether we would see the same effects in a group of participant reporting feeling lonely often. Testing the same mindfulness programme in a sample of people with higher ratings of loneliness is a must to allow for definitive conclusions regarding the usefulness of the intervention.

The use of active components in all three groups serves as a strength of the study, but it’s essential that this intervention is tested in people with higher levels of loneliness before we can come to any concrete conclusions.
Implications for practice
The results suggest that mindfulness could be another way of helping people struggling with frequent feelings of loneliness. In a field with no clear consensus about what is the best way to help lonely people, the results from this study adds to our toolbox of potential techniques and methods to be used. With the app-delivered guidance used in this study, the potential for widespread and inexpensive access would seem to be high. However, it is important to note that the results need to be replicated with participants where loneliness is a larger concern.
The ongoing pandemic and its impact on mental health has made the need for methods of dealing with loneliness a priority, and the use of mindfulness is an interesting candidate. It is not known whether the effects found in the study would be similar in the current environment with calls for social distancing and heavy regulation on where and when we can meet people. While mindfulness itself can be practiced alone at home, it is unclear whether using the method as a means for regulating one’s emotions can reduce loneliness in and of itself, or whether the benefits can only be seen when it is used a tool for achieving more frequent and more fulfilling interactions with others. The theoretical view described by the authors suggested that the second alternative may be more likely, but this has not been investigated. This angle is an interesting avenue of research for the future and one that might be worth looking into, both to help with the immediate needs during the Covid-19 pandemic, but also in the long-term.

We can add mindfulness to the list of promising candidates for reducing loneliness, but more studies are needed before we can recommend its use in clinical practice.
Reducing loneliness to alleviate and prevent anxiety and depression – our Active Ingredients review, Dr Eiluned Pearce
Our team was commissioned by The Wellcome Trust to look at reducing loneliness as a potential active ingredient in both alleviating and preventing anxiety and depression in young people aged 14-24.
Loneliness is relatively common in young people (DCMS 2017) and loneliness during childhood has been found to predict depression and emotional symptoms up to 24 years later (Lempinen et al 2018, Qualter et al 2010). It has also been found that loneliness is reciprocally associated with social anxiety over time in adolescents (Maes et al 2019). This suggests that by intervening to address loneliness, we may have the potential to both prevent the onset of anxiety and depression, and to help those already experiencing mental ill-health to feel less lonely.
Our research questions were:
- In which ways and in which contexts do existing interventions to address loneliness have the potential to reduce anxiety or depression in 14-24 year-olds and why?
- In which ways, in which contexts and for whom do they not work and why?
To answer these questions we brought together evidence from 27 academic studies (all published except one PhD thesis) reporting quantitative and/or qualitative data. To be included in our review these studies needed to include outcome measures of both loneliness and mental health. To complement these intervention studies we also incorporated evidence from 25 websites and reports from community and policy organisations such as the Office of National Statistics, The Children’s Society, The Co-op Foundation, the Department for Digital, Culture, Media and Sport for Civil Society, and the Mental Health Foundation, as well as 2 master’s dissertations that reported interviews with staff from charities working with young people. For the academic literature we ran systematic searches informed by consultations with academic experts from diverse disciplines including cognitive neuroscience, social work, the built environment, digital technology, health economics, arts and health and epidemiology. We also worked closely with young people (aged 18-25) in our Lived Experience Advisory Group (LEAG), who helped focus our searches of the literature, and shared their experiences of loneliness and mental ill-health and what had helped them overcome these challenges.
By drawing together these lived experience insights, perspectives from charities on providing services and support to young people, and evidence from academic research, we generated an exploratory framework (see the simplified version below) to summarise strategies for addressing loneliness and reducing anxiety and depression that may warrant future development. This framework was developed iteratively with feedback from the LEAG.
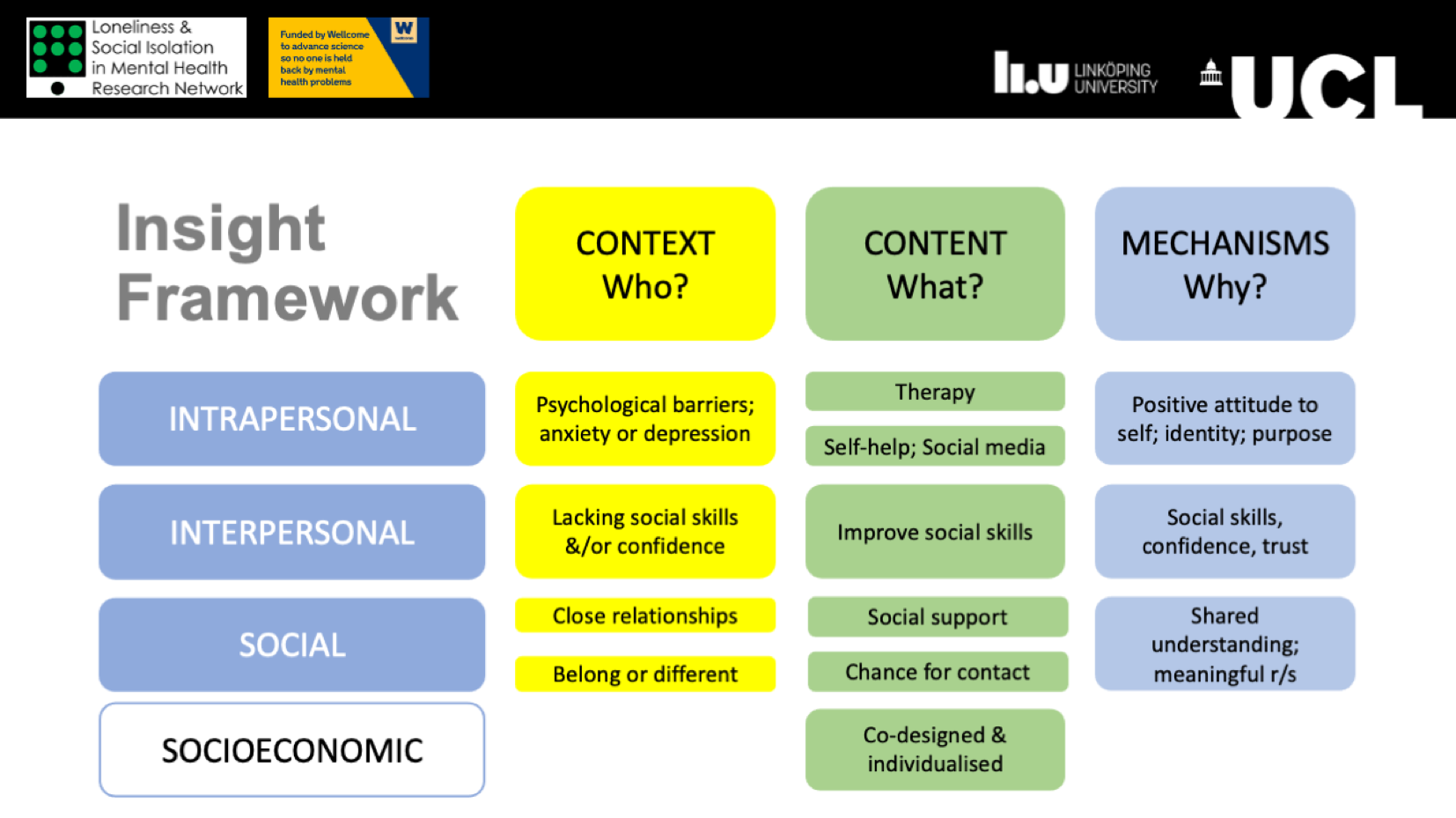
Our active ingredients review developed a framework of interventions for potential future development to address loneliness, anxiety and depression in young people. View full-size image.
Based on our research questions, we synthesised three main constructs from the evidence: (1) ‘context’ i.e. who interventions might work for – in terms of different causes of loneliness, (2) ‘content’ or the key elements of interventions, and (3) ‘mechanisms of action’ or why certain elements might be effective for particular young people.
We then synthesised three cross-cutting constructs from the evidence: intrapersonal, interpersonal and social constructs.
- ‘Intrapersonal factors’ underlying loneliness are psychological barriers such as not trusting others, low self-esteem, and whether an individual is experiencing anxiety or depression. ‘Intrapersonal Strategies’ include, for example, Cognitive Behavioural Therapy (CBT) and the mindfulness intervention discussed above, or Self-help Strategies like self-help apps, sport, or using social media. Plausible ‘Intrapersonal Mechanisms’ are creating more positive ways of looking at themselves and others, building purpose and identity. The importance of acceptance of one’s experiences reported by Lindsay et al (2019) is another potential intrapersonal mechanism.
- Interpersonal Factors underlying loneliness are lacking social skills and confidence, and Interpersonal Strategies aim to improve those social skills, which may work through building social skills, confidence and trust.
- Social Factors are lacking close relationships with friends or family or not feeling part of a wider social network or community, and Social Strategies include increasing social support e.g. through peer support groups or mentors, or providing opportunities for social engagements for example through music-making or playing sports. These strategies can allow individuals to build meaningful relationships and realise that they aren’t the only ones feeling like they do.
- There are also socioeconomic factors underlying loneliness, but we focused on these intrapersonal, interpersonal and social pathways in our review.

This new #ActiveIngredientsMH review synthesised three cross-cutting constructs from the loneliness and mental heath literature: intrapersonal, interpersonal and social factors.
From the evidence and consulting with the LEAG, we found that potential barriers (i.e. what factors might mean that an intervention might not work for someone) include individual-level psychological barriers such as not wanting to be a burden or situational barriers like work or caring responsibilities, practical barriers such as not having digital, physical or financial access to services and resources, and social barriers such as stigma or an unsupportive home environment.
The LEAG and charity workers talked about strategies needing to be co-designed to fit the needs of the individual, and interventions may need to incorporate multiple Content elements from the framework to be effective. For example, the online Entourage platform uses a strength-based cognitive therapy approach to helping young people overcome social anxiety but also has peer and professional mentors to provide social support (Rice et al 2020). The few studies that measured loneliness outcomes after social skills training were targeted at individuals with Autism Spectrum Disorder or social anxiety, so we don’t know whether this approach is more broadly applicable. Changing thinking around attitudes to self and others through therapy, and building trust through having ongoing social support, seemed to help young people already experiencing anxiety or depression. Having supportive peer groups that had shared experience, for example hospitalised young people doing music therapy together, or online forums for depressed university students, seemed to help reduce loneliness. The key mechanism of action here was ‘recognising that shared experience’ and realising that you’re not the only person feeling that way. It’s plausible that some of these groups may also have helped provide identity and inadvertently help build social skills and social confidence. The importance of co-design and opportunities to build trust were also highlighted in some of the other Active Ingredient projects looking at neighbourhood cohesion and social relationships.
Limitations
Many of the studies we looked at were small-scale feasibility or pilot studies, so the evidence of effectiveness of these interventions is still lacking. Moreover, as pointed out in relation to Lindsay et al (2019) above, interventions often do not target lonely individuals, so more research needs to look at what helps those already feeling lonely, particularly those whose loneliness is chronic rather than transitory. We did not find any mindfulness interventions for loneliness that also looked at mental ill-health in young people, although Zhang et al (2018) did find encouraging results in college students (this study was excluded from our study because it looked only at loneliness, and not anxiety or depression). Future studies would benefit from including outcome measures of anxiety and depression as well as loneliness, and looking at these over time.
Conclusion
Overall, the most promising approach to addressing loneliness and reducing anxiety and depression in young people may be interventions that flexibly combine (or offer the choice of) some form of cognitive therapy (perhaps including mindfulness, although Lindsay et al 2019 did not focus on young people), sustained social support (perhaps one-to-one for those already experiencing severe anxiety or depression), and peer groups that share specific shared experiences such as bereavement, or being overseas students.
Statement of interests
No potential conflicts of interest to report.
Links
Primary paper
Lindsay, E. K., Young, S., Brown, K. W., Smyth, J. M., & Creswell, J. D. (2019). Mindfulness training reduces loneliness and increases social contact in a randomized controlled trial. Proceedings of the National Academy of Sciences, 116, 3488-3493. doi:10.1073/pnas.1813588116
Other references
Department for Digital Culture Media and Sport and Office for Civil Society (2017) Community Life Online and Paper Survey Technical Report 2016-2017.
Khoury, B., Lecomte, T., Fortin, G., Masse, M., Therien, P., Bouchard, V., . . . Hofmann, S. G. (2013). Mindfulness-based therapy: A comprehensive meta-analysis. Clinical Psychology Review, 33, 763-771. doi:https://doi.org/10.1016/j.cpr.2013.05.005
Lempinen L, Junttila N, Sourander A. (2018) Loneliness and friendships among eight-year-old children: time-trends over a 24-year period. J Child Psychol Psychiatry Allied Discip. 59(2):171–9.
Maes M, Nelemans SA, Danneel S, Fernández-Castilla B, Van den Noortgate W, Goossens L, et al. (2019) Loneliness and social anxiety across childhood and adolescence: Multilevel meta-analyses of cross-sectional and longitudinal associations. Dev Psychol. 55(7):1548–65.
Masi, C. M., Chen, H.-Y., Hawkley, L. C., & Cacioppo, J. T. (2011). A meta-analysis of interventions to reduce loneliness. Personality and Social Psychology Review, 15, 219-266. doi:10.1177/1088868310377394
Qualter P, Brown SL, Munn P, Rotenberg KJ. (2010) Childhood loneliness as a predictor of adolescent depressive symptoms: An 8-year longitudinal study. Eur Child Adolesc Psychiatry. 19(6):493–501.
Rice S, O’Bree B, Wilson M, McEnery C, Lim MH, Hamilton M, et al. (2020) Leveraging the social network for treatment of social anxiety: Pilot study of a youth-specific digital intervention with a focus on engagement of young men. Internet Interv. 20:100323.
Spithoven, A. W. M., Bijttebier, P., & Goossens, L. (2017). It is all in their mind: A review on information processing bias in lonely individuals. Clinical Psychology Review, 58, 97-114. doi:10.1016/j.cpr.2017.10.003
Zhang, N., Fan, F., Huang, S., Rodriguez, M.A. (2010) Mindfulness training for loneliness among Chinese college students: A pilot randomized controlled trial. International Journal of Psychology 53(5): 373-378. DOI: 10.1002/ijop.12394.
