
Immediate placement of dental implants into fresh extraction sockets has for some time been an established surgical technique. The theory is that it preserves alveolar ridge, reduces morbidity, and is more acceptable to the patient. However, there may also be disadvantages such as reduced implant survival, unfavourable changes in the hard/soft tissue and extended treatment times. To standardise the type of implant placement they have been classified into four types:
- Immediate placement (type 1).
- Early placement with soft tissue healing (type 2).
- Early placement with partial bone healing (type 3).
- Late placement (type 4).
The research question for this systematic review and meta-analysis was: ‘‘Do immediately inserted implants perform similarly to implants that are inserted into a healed socket?’’
Methods
This review was performed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement and registered with PROSPERO.
The population (P) was patients who had undergone osseointegrated implant insertion into fresh extraction sockets (I) or healed sockets (C). The primary outcome (O) evaluated was implant survival rate. Marginal bone loss, primary implant stability, and soft tissue changes were considered secondary outcomes. The following inclusion criteria were applied: Randomised controlled or prospective studies in English. More than five implants per group with a minimum of six months follow-up. Exclusion criteria were animal and in vitro studies, simple evaluations without comparators or analyses of loading protocols.
Two researchers independently selected and screened articles PubMed/Medline, Embase, and Cochrane databases and manually searched relevant specialist journals. Quality assessment was undertaken using the Jadad scale and Cochrane Collaboration’s tool for assessing risk of bias.
Result
- The systematic Search found 30 papers out of 3049 which fulfilled the inclusion criteria. On the Jadad risk of bias assessment only 8/30 studies were evaluated as high quality.
- Meta-analysis results (Primary outcomes)
| Relative risk
(95% Confidence Interval) |
Probability | |
| Survival favours healed sockets | 2.49, (1.44 – 4.29) | p = 0.001 |
| Type 1 compared with type 2 | 1.45, (0.53 – 3.98). | p = 0.47 |
| Type 1 compared with type 3 | 5.25, (1.67 – 16.49) | p = 0.005 |
| Type 1 compared with type 4 | 2.86, (1.22 – 6.70) | p = 0.02 |
- There were no statistical differences in the secondary outcomes.
Conclusion
The authors concluded:-
In conclusion, immediate implant insertion should be performed with caution because implant survival rates are significantly lower than with implants inserted into healed sockets.
Comments
My intuition tells me that the authors may have the right answer but the evidence they present does not support this for various methodological reasons. The major problem is that the survival data is of relatively short duration and heterogeneous with a mean follow-up being 24 months, median 18 months and a mode of 12 months.
Clinicians mostly will only be interested in long-term data (60 months plus). Focusing on just these longer-term studies papers in the review just leaves three papers (Cooper et al 2014, Polizzi et al 2000 and Raes et al 2016) , so a second Raes paper (Raes et al 2013) with a stated 52 months follow up and the 2015 Oxby paper with 55 months follow up were reviewed and meta-analysed.
Looking at these research papers with the longest follow-up is simpler to appraise than the 30 the authors included. Full texts were obtained and the following conclusions made:
- The Raes paper (Raes et al 2013) states only 52 weeks follow-up not 52 months as in the review, which is quite important if we are meant to be looking a survival studies.
- In the Polizzi paper (Polizzi et al 2000) there is no randomisation between the healed and fresh extraction sockets.
- The Oxby paper reads as though it is retrospective review and 25% of the sample was excluded after implant placement as the loading protocol exceeded 60 days (this group could possibly contain the failures?). Not all the implants were reviewed at 60 months (38/182 were reviewed between 36-48 months, 114/182 between 49-60 months and 30/182 between 60-63 months).
- Lost to follow (LTF) up in the studies varies from 13% – 40%. The authors classified the LFT patients as missing completely at random to optimise the survival data.
The 2013 Raes paper was therefore excluded as the follow-up was too short, and the Oxby paper as a retrospective study (exclusion criteria). The remaining studies were included in a meta-analysis. Group a. is the data as published in the systematic review and Group b. where LTF is considered in the calculations as a failure.
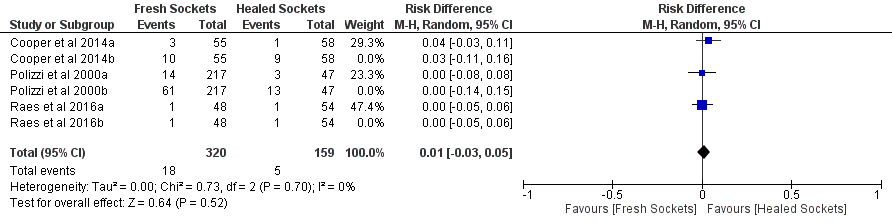
Fig.1 shows the new risk ratio (RR) for the long-term data has reduced from 2.49 to 1.28. If missing data is considered as a failure the RR drops to 1.06 (Fig. 2). An interesting observation is that the risk difference for Group a (Fig. 3) is 0.01.
Fig. 1. Forest plot for the event ‘60-month implants survival rates’ for Group a.
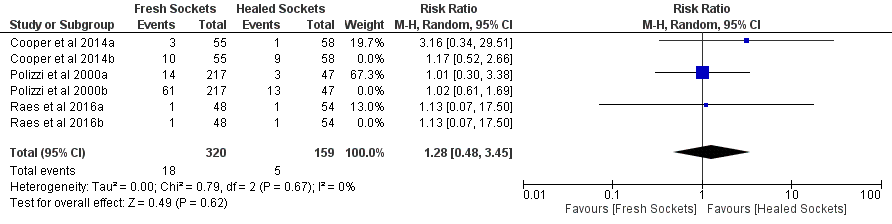
Fig. 2. Forest plot for the event ‘60-month implants survival rates’ for Group b.
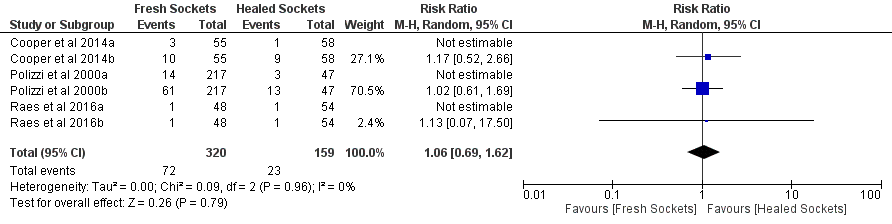
Fig. 3. Forest plot for the Risk Difference ‘60 month implants survival rates’ for Group a.
In conclusion from this data there is no difference between techniques, possibly due to the ability to select cases rather than a true randomisation. One interesting point is that long-term survival for fresh v. healed was 94.4 and 96.9; if missing data is considered a failure 5-year survival drops by a further 15%. As usual the truth lies somewhere in between.
Links
Primary paper
Mello CC, Lemos CAA, Verri FR, Dos Santos DM, Goiato MC, Pellizzer EP.Immediate implant placement into fresh extraction sockets versus delayed implants into healed sockets: A systematic review and meta-analysis. Int J Oral Maxillofac Surg. 2017 May 3. pii: S0901-5027(17)31361-9. doi: 10.1016/j.ijom.2017.03.016. [Epub ahead of print] Review. PubMed PMID: 28478869.
Other references
Cooper LF, Reside GJ, Raes F, Garriga JS, Tarrida LG, Wiltfang J, Kern M, De Bruyn H. Immediate provisionalization of dental implants placed in healed alveolar ridges and extraction sockets: a 5-year prospective evaluation. Int J Oral Maxillofac Implants. 2014 May-Jun;29(3):709-17.
Polizzi G, Grunder U, Goené R, Hatano N, Henry P, Jackson WJ, Kawamura K, Renouard F, Rosenberg R, Triplett G, Werbitt M, Lithner B. Immediate and delayed implant placement into extraction sockets: a 5-year report. Clin Implant Dent Relat Res. 2000;2(2):93-9.
Raes S, Raes F, Cooper L, Giner Tarrida L, Vervaeke S, Cosyn J, De Bruyn H. Oral health-related quality of life changes after placement of immediately loaded single implants in healed alveolar ridges or extraction sockets: a 5-year prospective follow-up study. Clin Oral Implants Res. 2017 Jun;28(6):662-667. Epub 2016 May 22.
Oxby G, Oxby F, Oxby J, Saltvik T, Nilsson P. Early Loading of Fluoridated Implants Placed in Fresh Extraction Sockets and Healed Bone: A 3- to 5-Year Clinical and Radiographic Follow-Up Study of 39 Consecutive Patients. Clin Implant Dent Relat Res. 2015 Oct;17(5):898-907.
Raes F, Cosyn J, De Bruyn H. Clinical, aesthetic, and patient-related outcome of immediately loaded single implants in the anterior maxilla: a prospective study in extraction sockets, healed ridges, and grafted sites. Clin Implant Dent Relat Res. 2013 Dec;15(6):819-35.
Dental Elf -12th Dec 2014
https://www.nationalelfservice.net/dentistry/restorative-dentistry/dental-implants-placed-in-fresh-sockets-have-higher-failure-rates-suggests-review/

[…] https://www.nationalelfservice.net/dentistry/restorative-dentistry/dental-implant-placement-fresh-ex… […]
[…] Dental implant placement into fresh extraction sockets […]